Pathogenesis of Adhesions and the Risk of Complications
The clinical burden of adhesions is extensive
Adhesions and their caused complications have already been known for 150 years. Bryant published one of the first data on adhesions in 1872, as he described a patient case that showed intestinal obstruction caused by intra-abdominal adhesions after removal of an ovarian tumor. 20 Only a few years later Dembrowski published study data on an animal model which already confirmed a correlation of foreign bodies and adhesions. 22
Intra-abdominal adhesions arise from aberrant peritoneal wound healing processes, any mesothelial damage by surgical trauma or bacterial inflammation can lead to their formation. 21
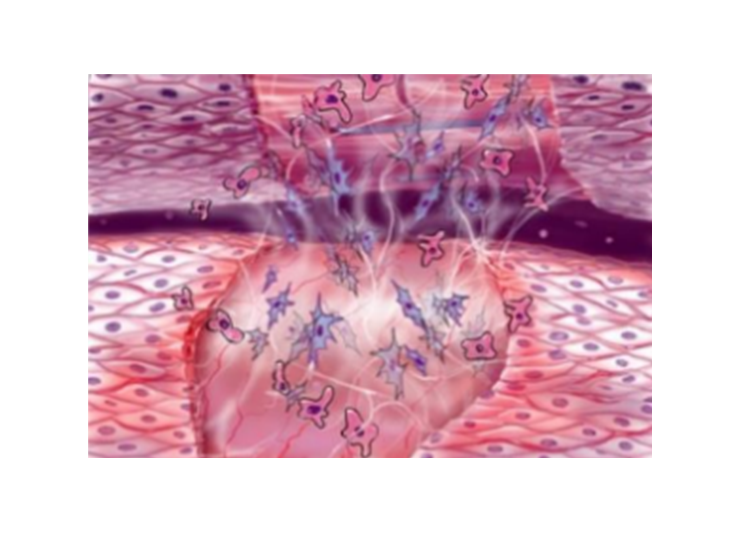

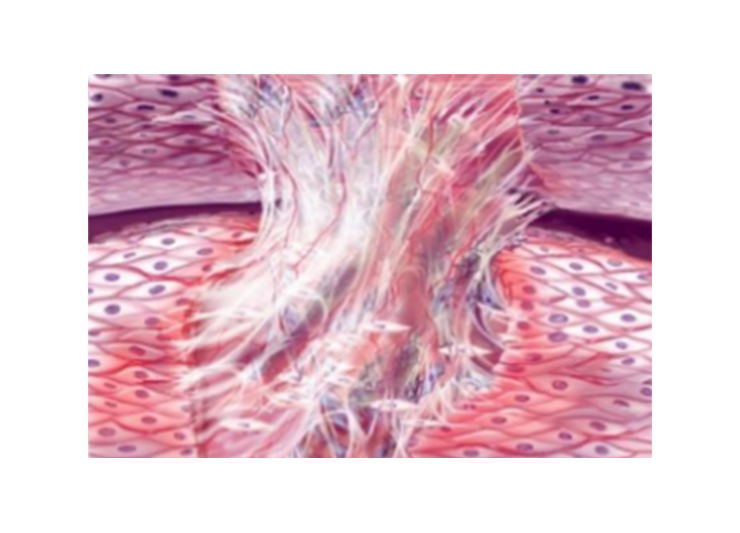
Studies imply that a source of adhesion formation is the pathological reduction of fibrinolysis capacity. 17
The process of adhesion formation is a multifactor process, while fibrinolysis capacity is one of the suggested influencers which is affected by multiple factors. 17
Detailed insights on the development and causes of adhesions are not yet fully confirmed but a study published in 2021 found that macrophages play a significant role in developing adhesions. 38
Adhesion types
Adhesions appear in two different types, either they are congenital adhesions which “arise during physiological organogenesis”17 or are caused inflammatory diseases such as endometriosis, peritonitis or inflammatory following radiotherapy or peritoneal dialysis. 23-25
The second type is acquired adhesions which arise after surgeries and appear in up to 100% of patients postoperatively.4
Consequences of Adhesions
Unlike other postop complications, such as wound infection or anastomotic leakage, consequences of adhesions include possible lifelong risks 31-32

- Major cause of small bowel obstruction (74% are adhesion related) 2
- Major contributory factor to chronic pelvic pain (up to 40% of cases) 28
- Chronic lower abdominal pain severely impairs the quality of life of those affected and forms the indication for 30% to 50% of all laparoscopies and 5% of hysterectomies 29
Patients in high risk of postoperative adhesions
Adhesions appear in up to 100% of patients after gynecological surgery. 4 When undergoing adnexal surgery patients develop ovarian adhesions even in 90% of cases. 26

Specific patient factors and certain surgeries increase the risk of adhesions development4
- Patients who already had adnexal or bowel surgery
- Patients with inflammatory disease
- Patients with Endometriosis 27
- Patients undergoing Myomectomies 27, Hysterectomies 27, and Adhesiolysis 27
Diagnosis
Adhesions can be confidently diagnosed intraoperatively while no other imaging can guarantee a secure clear diagnosis. Ultrasound or MRI could imply diagnosing adhesions by detecting reduced movement in the abdominal cavity due to connecting adhesions. 17